

The last couple of months have been eventful on the cannabis legalisation front. We learned from Bloomberg that the US Department of Health and Human Services (HHS) wants to kind of, maybe, potentially turn its eyes towards cannabis legalisation.
In August, the HHS sent a letter to the Drug Enforcement Agency (DEA) recommending reclassifying cannabis from Schedule I of the Controlled Substances Act (CSA) to Schedule III. The report includes confirmation from a DEA spokesperson that the Agency received the recommendation letter.
This is excellent news.
If the proposal gets approved, it would mark the most significant change in federal marijuana policy since the prohibition started in 1937. It’s a big step back from the harsh anti-drug measures that have shaped American drug policies for the past 50 years.
The recommendation comes after President Joe Biden’s order last October. He pardoned 6,500 people convicted of minor marijuana offences (although none were still in prison) and urged his administration to reconsider the plant’s legal status. Now, the proposal is heading to the Justice Department, which might give its approval before the next presidential election. Many see this move as a major shift in how the United States views and treats marijuana on a federal level.
Although we are not yet talking about legal cannabis, the potential reclassification has some significant implications regarding its acceptance as a medical treatment. It can also help marijuana businesses get a tax break and improve their bottom line while also giving a possible path toward national legalisation.
All of this got us thinking about what exactly would change if marijuana is reclassified to Schedule III.
Understanding the current classification and what it does – The Controlled Substances Act
First, let’s review the basics: what the current cannabis classification is and what it means.
Controlled Substances Act (CSA or the Act)
The US Centers for Disease Control and Prevention (CDC) found that in 2019, 48.6% of Americans had taken one or more prescription drugs in the last month. At the same time, both pharmaceutical and non-pharmaceutical drugs can impact public health. 106,699 Americans lost their lives due to drug overdoses in 2021. In theory, the Controlled Substances Act seeks to remedy these considerations. In reality, however, the 50-year-old schedule system is a mess. It includes both FDA-regulated pharmaceuticals and street drugs subjected to law enforcement.
In 1970, President Richard Nixon passed the CSA into law. It creates a unified federal policy that regulates all aspects of specific substances – manufacture, importation, possession, use, and distribution. It deals with drugs, whether medical or recreational, legally or illicitly distributed, that are found to pose certain health risks to the public.
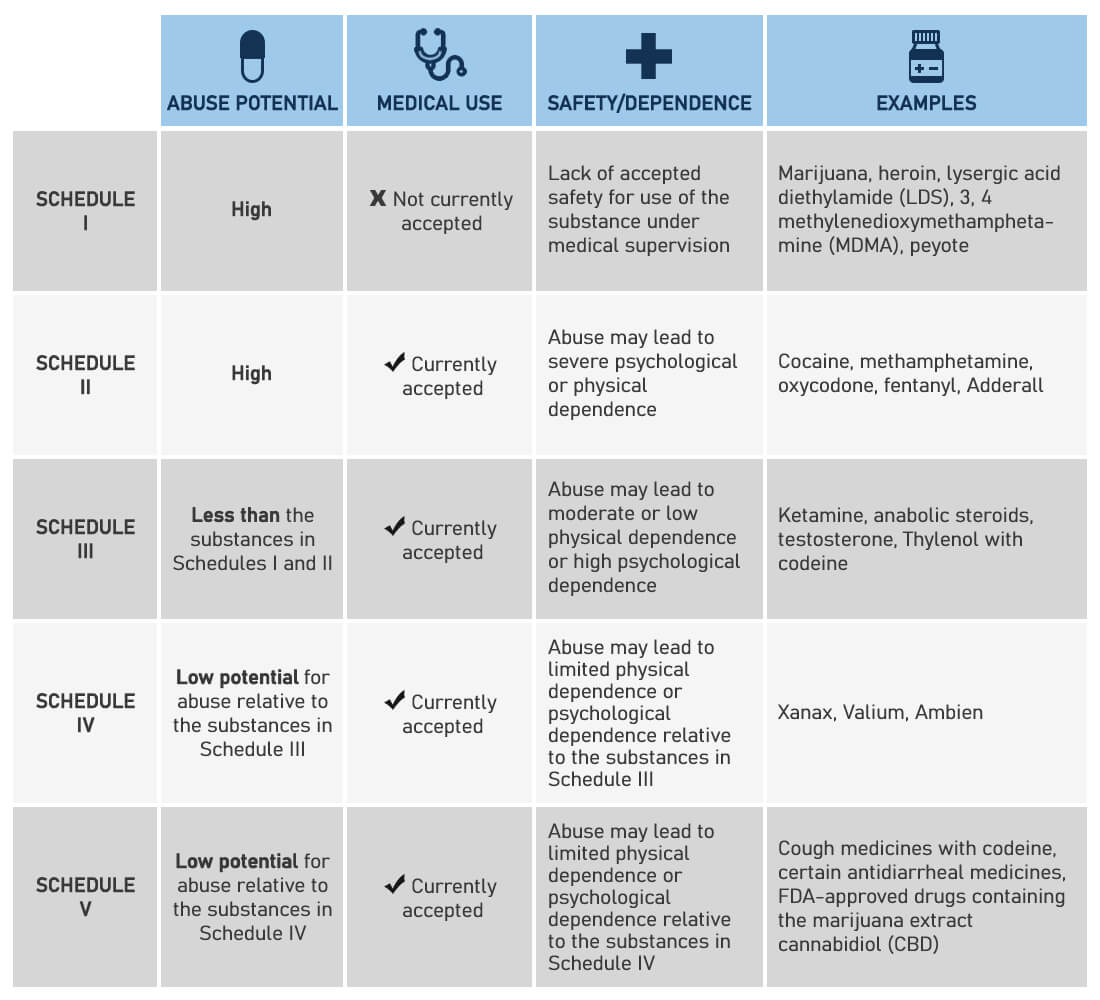
It places those drugs into five categories or Schedules based on their risk to public health, accepted medical use, and potential for abuse and dependence.
The CSA System
Schedule I
- The substances have a high potential for abuse. They have no currently accepted medical use in treatment. There is a lack of accepted safety use under medical supervision.
- Examples: heroin, LSD, MDMA, and marijuana.
Schedule II
- The substances have a high potential for abuse. They currently have some accepted medical use in treatment or a currently accepted medical use with severe restrictions. Abuse may lead to severe psychological or physical dependence.
- Examples: morphine, phencyclidine (PCP), cocaine, methadone, fentanyl, and methamphetamine.
Schedule III
- The substances have less potential for abuse than those in Schedules I and II. They currently have accepted medical use in treatment in the United States. Abuse may lead to moderate or low physical dependence or high psychological dependence.
- Examples: anabolic steroids, codeine products with aspirin or acetaminophen, and some barbiturates.
Schedule IV
- The substances have a low potential for abuse relative to those in Schedule III. They have a currently accepted medical use in treatment. Abuse may lead to limited physical dependence or psychological dependence relative to those in Schedule III.
- Examples: alprazolam, clonazepam, and diazepam.
Schedule V
- The substances have a low potential for abuse relative to Schedule IV. They have currently accepted medical use in treatment. Abuse may lead to limited physical dependence or psychological dependence relative to those in Schedule IV.
- Examples: cough medicines with codeine.
As you can see, Schedule I is the most restrictive category. Because of this, engaging with cannabis in any way can result in federal criminal penalties. Even in states where cannabis is legal. Additionally, Schedule I prohibits any form of medical or scientific research.
The primary agency responsible for implementing and enforcing the CSA is the Drug Enforcement Administration. It was established in 1973, taking over the federal Bureau of Narcotics. Only the DEA, the US Congress, and the Food and Drug Administration (FDA) have the power to add, remove or reschedule substances.
If you want to learn more about the legal status of cannabis, please read our article The Legal Landscape of Cannabis Worldwide.
Now that you know what the CSA is, you might ask why cannabis is classified as Schedule I.
Well, as you probably guessed, the answer is complicated. Cannabis regulation is steeped in decades of propaganda, racism, and public misconceptions.
Many believe that the modern cannabis policy started with the Control Substances Act, but its principal predecessor is the Marijuana Tax Act (MTA) from 1937, which intended to ban marijuana on a federal level.
It’s debatable whether the anti-cannabis campaign that led to the MTA’s passage was for a few people’s personal benefit, as neither the MTA nor its successor, the CSA, were founded on serious scientific inquiry and real policy or moral considerations.
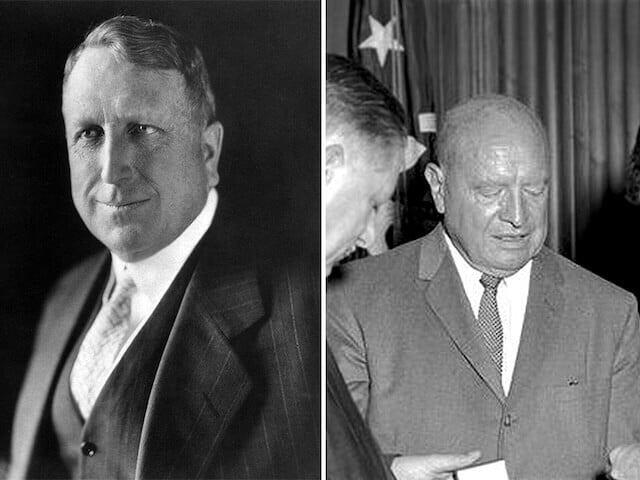
The main culprits: William Hearst and Harry Anslinger
And it’s all because of two people: William Randolf Hearst and Harry J. Anslinger.
William Randolf Hearst was the first media mogul in the United States. He was also a ruthless businessman with a strong dislike of marginalised groups, Mexican immigrants in particular.
Harry J. Anslinger was a bureaucrat who became the first director of the Federal Bureau of Narcotics. An avid prohibitionist, after the re-legalisation of alcohol, Anslinger found his true calling in the fight against cannabis. He also was an ardent racist. One of his most famous quotes is: “Reefer makes darkies think they’re as good as white men. The primary reason to outlaw marijuana is its effect on the degenerate races.”
Hearst and Anslinger used their vast resources to push nationwide anti-cannabis propaganda for one simple reason: money and power.
Hearst spent his life building his media empire while also heavily investing in the timber business. This makes sense since timber fibre is used to produce paper. However, hemp’s competition threatened Hearst’s business because its fibre is better for making paper. Also, hemp grows faster than trees.
Since Hearst had access to every segment of the population through his popular newspapers and magazines, he aggressively used the outlets to change public opinion. He spread misinformation about marijuana users and dependency.
On the other hand, Anslinger saw cannabis as the moral depravity of his time. A personal distaste for jazz music fueled his extreme racist beliefs. His view of the cannabis users was that “most are Negroes, Hispanics, Filipinos, and entertainers. Their Satanic music, jazz, and swing result from marijuana use. This marijuana causes white women to seek sexual relations with Negroes, entertainers and any others.” Because of this, he used Hearst’s media network to ram cannabis prohibition down people’s throats.
At the same time, Anslinger’s ambition had a practical side. He also sought to create a haven for two emerging industries at the time, which saw weed and hemp as direct threats to their commercial interests. Those were the pharmaceutical industry, which was gaining speed with the introduction of penicillin and the synthetic industry, which began producing plastics.
He achieved this by eliminating the perception of cannabis as an effective natural medicine and pushing for a ban on commercial hemp production.
From Cannabis to Marijuana
Hearst and Anslinger actually came up with the term Marijuana, rooted in Mexican-Spanish. They wanted to dissociate it from cannabis, as it was known in the US, by tying it to the influx of Mexican immigrants. At the same time, they were demonising the plant as a dangerous and addictive drug that caused Black Americans, Mexicans, and members of the lower classes to commit crimes. For them, it was the leading cause of moral decay, social unrest, and the primary threat to white America.
Anti-drug advocates, supported by Anslinger, raised alarms about the so-called Marijuana Menace, leading to a shift in public perception.
Fear of the plant peaked with the propaganda film Reefer Madness, released in 1936. The film warned parents of the supposed dangers of cannabis use, portraying various horrible incidents that occur to a group of teenagers all because they smoked pot. Today, the film is a cult classic and an example of the ridiculous exaggerations of the plant’s effects that many people believed.
That way, Hearst and Ansligner were able to outlaw cannabis for their financial and political interests. Their efforts culminated in the passing of the Marijuana Tax Act.
As a result, nobody really realised that this dangerous new drug, marijuana, was actually cannabis until it was federally prohibited.
The status quo continued for decades. By the 1970s, the US federal government under Richard Nixon had declared a full-on war on drugs, and weed was one of its primary targets.
Rise of the counterculture and the turn of the 19th century
The government’s actions of course pushed cannabis underground, spawning an active opposition and a vibrant counterculture.
Despite the government’s efforts, people continued to use marijuana recreationally. Many artists and activists used their platforms to speak out against prohibition. Marijuana also became part of the hippie and anti-war movements, and a new major shift in public consciousness began to sprout.
Eventually, in 1996, California voters led the charge and passed Proposition 215, which legalised medical cannabis in the state. This was a significant turning point in the legalisation movement, which sparked a wave of similar initiatives nationwide.
With the turn of the 21st century, different states slowly began reversing their cannabis policy restrictions. First by decriminalising small amounts for personal use and then gradually legalising medical cannabis. This momentum continued to build, and by 2012, Colorado and Washington became the first states to legalise recreational cannabis for adults.
This brings us to the present times. Today, two-thirds of Americans support cannabis legalisation. Thirty-eight states offer medical cannabis programs, and 23 have legalised some form of recreational use.
Although the Controlled Substances Act still reigns supreme on a federal level, its role in regulating marijuana is becoming increasingly redundant. Legislatures and local governments constantly consider ways to remedy the conflict between federal and state laws and adapt the CSA to a booming cannabis industry.
This is where cannabis rescheduling might be an important first step towards federal legalisation.
Marijuana is reclassified to Schedule III. What now?
Considering the recent developments, let’s see now what would change if cannabis is reclassified as Schedule III.
In general, Schedule III drugs such as ketamine and Tylenol are FDA-approved, uniformly regulated by the federal government, and are legally available only by prescription. The same will apply to cannabis. Having this in mind, Schedule III will bring three meaningful changes.
- It will allow medical and scientific research. This means federal programs and funding, research opportunities, and international cooperation.
- It will finally end the stigma surrounding cannabis. Although most people are already familiar with cannabis’s therapeutic benefits, many are still not convinced precisely because of the government’s stance. It will bring marijuana “out in the open” and legitimise the plant as a viable treatment option for various conditions.
- It will help businesses and boost investments by alleviating some restrictions plaguing the industry. Specifically, it will end a tax rule known as 280E that the cannabis industry hates.
As for recreational cannabis use, unfortunately, Schedule III would not legalise the sale of marijuana for recreational use, nor would it legalise marijuana products – such as flower, edibles, vapes, topicals, or anything besides FDA-tested and approved drugs in specific forms.
Expanding medical and scientific research on cannabis
Historically, it has been almost impossible to research cannabis due to a required permit from the DEA. Getting it is incredibly challenging since the CSA deems weed too dangerous to study with human subjects, even under the supervision of doctors and health care professionals.

In addition, because of the heavy restrictions imposed by Schedule I, locating and possessing marijuana for research is also a burden. Researchers are only allowed to procure it from a single farm at the University of Mississippi. Their plants, however, bear little resemblance to the high-potency products many of us purchase in state-legal markets.
While substances under Schedule III are still controlled, it will open up many research pathways, allowing scientists to understand better the cannabis plant and its interactions with the human body. It will also enable them to conduct large double-blind peer-reviewed studies, which have been the gold standard for FDA’s medicine approval since the mid-1960s.
This, in turn, will stimulate the creation of federal research programs, bring funding opportunities, and encourage international cooperation. Additionally, the government will need to update its records and provide science-based knowledge to the public.
Pharmaceutical companies and drug manufacturers will be able to develop new drugs from cannabinoids – the active compounds in cannabis. Once those drugs are developed, consumers can get them from pharmacies with a prescription from a doctor.
Industry and banking: unlocking financial services and tax benefits
The most significant change the reclassification would bring is the removal of the notorious tax rule 280E.
Under Section 280E of the Internal Revenue Code, the federal law states that businesses dealing with Schedule I or II controlled substances, such as marijuana, can’t get tax deductions or credits. Because marijuana is currently Schedule I, businesses can’t subtract important costs from their taxable income on federal tax returns. This means marijuana business owners have to pay taxes on their income without being able to reduce them by accounting for their business expenses. Rescheduling marijuana will change this rule, giving companies a tax advantage used by “normal” businesses.
Rescheduling will also pave the way for the so-called SAFER Banking Act, offering a partial solution to the banking problem that plagues the industry. On September 21, a bipartisan group of senators introduced the legislation named the Secure and Fair Enforcement Regulation (SAFER) Banking Act. The Senate Committee on Banking, Housing and Urban Affairs approved it. Titled initially the Secure and Fair Enforcement (SAFE) Banking Act, the new version of the bipartisan legislation would make it easier for cannabis companies to access traditional banking services.
Because it’s federally illegal, banks generally want nothing to do with cannabis. As a result, businesses don’t have access to bank accounts, credit cards and other financial services. This forces the owners to operate strictly in cash, leaving them and their customers vulnerable to crime. Not to mention that it opens ways for money laundering.
While federal legalisation would provide the most complete solution, The SAFER Banking Act could be an intermediate step to ease financial hurdles for the industry, allowing it to operate more transparently within the existing financial system. This will also attract more investors and entrepreneurs to the market and make it easier to acquire capital.
Impact on public perception: ending the stigma and recognising cannabis’s medical value
Another significant change from the reclassification will be that the US will finally recognise the medical value of cannabis at a federal level. This will go a long way toward changing public perception and reversing decades of government propaganda about its potential and safety. It will also increase acceptance among those who remain sceptical about its medical use. This may help reduce incarcerations and criminal sentences.
As you can see, rescheduling cannabis represents a middle ground for the government to adapt its bureaucracy to the booming industry without throwing things into chaos. This would be an excellent test to determine how a federal regulation would look and potentially offer solutions on fully legalising cannabis.
Potential Challenges
Still, a lot needs to happen before Schedule III becomes a reality. There will be issues with the current legislation, existing state laws, and international treaties. There will also be regulatory challenges like setting dosing standards and quality control.
Adapting US Federal Legislation to the new Schedule
Currently, the US government is stuck in a bureaucratic circle.

In 2016, the DEA concluded that “marijuana has no ‘currently accepted medical use’ because… the drug’s chemistry is not known and reproducible; there are no adequate safety studies; there are no adequate and well-controlled studies proving efficacy; qualified experts do not accept the drug; and the scientific evidence is not widely available.”
This, however, is precisely because cannabis is Schedule I. So, you have a real Catch-22 moment, where marijuana is a Schedule I drug because there are no accepted scientific studies. And there are no accepted scientific studies because marijuana is a Schedule I drug.
A complicated administrative process makes this situation even worse.
In simpler terms, before HHS recommends reclassifying a drug, the Food and Drug Administration conducts a medical and scientific review using what is called an eight-factor analysis. It considers the potential for abuse of the drug, its history of abuse and the scientific evidence of its pharmacological effect. The FDA sends the review to HHS, which uses it as the basis of its recommendation to the DEA. That agency then conducts its own analysis, which involves issues beyond the scope of the health agencies. And this is even before the process reaches Congress.
After all this, if the authorities decide that rescheduling cannabis is appropriate, the federal government will still need to address conflicts with existing state laws.
Opponents of rescheduling note that it would do little to close the ever-growing gap between state and federal cannabis legislation, as it is not designed for a Schedule III drug.
Even as consumption rises, existing contradictions have made it very difficult for companies to participate in the industry and make money. For example, current laws confine cannabis businesses within the state where they operate. They can’t move their production because weed is federally illegal. This applies even if they want to export to states where it is legal. In addition, the highway system falls under federal jurisdiction, further complicating the situation. This means businesses are still committing a federal crime using the road network even if transporting goods within state lines.
So, if companies want to expand, they must set up shop in every state where they want to operate. Then, they have to go through the same registration process of obtaining permits, licences, etc. But the problems don’t end there. The lack of standardised rules from federal agencies for things like testing, dosage, labelling, and storage makes it even more challenging to work in multiple states due to the need to comply with a patchwork of sometimes draconian regulations.
Cannabis’s legal status won’t change under Schedule III
Schedule III won’t resolve these issues or cannabis’s legal status. It won’t end criminalisation – it will just rebrand it. Regardless of the medical program’s status, people will still be subject to criminal penalties for mere possession.
With the current cannabis classification, state industries exist because the DEA has chosen not to crack down on them. Schedule 3 substances are more loosely enforced than Schedule I, but they are still enforced. Whether cannabis is Schedule I or III, a state-licensed dispensary is still federally illegal, the same way an open fentanyl market is federally illegal. The difference is just a matter of enforcement priorities.
At the same time, patients for Schedule III pharmaceuticals need to renew their prescriptions every six months. For the industry to comply, it would require a major overhaul of the dispensary system as it currently operates. Although it’s more likely that businesses would be able to continue working as they currently do, that freedom would still be at the mercy of the feds rather than because marijuana is legal.
FDA Regulations and Big Pharma taking over
It’s very possible that in this complicated environment, the FDA may step in and revise the sort of hands-off approach it currently follows. The FDA can fully enforce regulations on cannabis as it does for all other Schedule III drugs. This could indicate significant changes in state markets. Local businesses might not be able to keep up, or at least they’ll be slow to respond, opening a way for Big Pharma to start taking over. In this unpleasant scenario, the pharmaceutical industry might eventually replace the current industry.
Compliance with International Treaties

Another element of cannabis rescheduling is how the decision would play out under international drug treaties. The DEA’s conclusion also states that “given United States obligations under international drug control treaties, marijuana cannot be placed in a schedule less restrictive than Schedule II.”
The Agency refers to the UN’s Single Convention on Narcotic Drugs from 1961. It introduces an identical scheduling system that ranks narcotic substances from most to least restrictive – Schedule IV, I, II and III, respectively. Schedule IV is the category of drugs considered particularly dangerous, have high levels of addiction, and have no medical benefits. Schedule I includes drugs that are limited to medical and scientific purposes.
The Convention is legally binding under the 1969 Vienna Convention on the Law of Treaties. It stipulates that a nation “may not circumscribe its obligations under the treaties by enacting a conflicting domestic law.”
However, the International Narcotics Control Board, created to ensure compliance, is limited to enforcement through diplomacy. It is also worth noting that Canada has not yet faced any sanctions, even though it federally legalised marijuana in 2017.
Conclusion
The path to Schedule III is complicated and chaotic. In addition, the rescheduling won’t resolve the underlying problems surrounding cannabis use and won’t legalise it federally. It will, however, offer a way forward. Its reclassification will finally end the public stigma by recognising its medical potential and allowing scientific research. It will also alleviate some of the financial burdens facing the industry.
To achieve this, the government will need to update its bureaucracy. It must also introduce regulations that protect small business owners while restricting Big Pharma’s reach.





Leave a Comment